
- Record: found
- Abstract: found
- Article: found
Does surgical treatment within 4 hours after trauma have an influence on neurological remission in patients with acute spinal cord injury?
Abstract
Background
The proper timing for surgery in patients with acute spinal cord injury is controversial. This study was conducted to detect if there is an advantage in early (within the first 4 hours after trauma) compared to late (between 4 and 24 hours after trauma) surgery on neurological outcome.
Methods
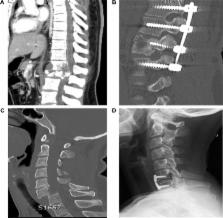
In this single institution prospective cohort study, data were analyzed from 51 spinal cord injured patients with an average age of 43.4 (±19.2) years. The influence of early (29 patients within the first 4 hours) as opposed to late (22 patients between 4 and 24 hours) decompression was evaluated by comparing data for neurological outcome. Patients of the study collectively suffered acute spinal fractures from C2 to L3 (cervical 39.2%, thoracic 29.4%, and lumbal 21.6%) or nonosseous lesions (9.8%). American Spinal Injury Association (ASIA) Impairment Scale (AIS) grades were assessed at time of admission and 6 months after trauma or longer depending on the time of release. Surgical treatment included early stabilization and decompression within 24 hours.
Results
No significant difference between improved neurological function, measured with the AIS, and an early or late surgery time can be seen ( P=0.402). Furthermore, binary logistic regression shows no significant difference between sex or age, and AIS improvement as possible confounders.
Conclusion
In our study, all patients with spinal cord injury were treated with spine stabilization and decompression within the first 24 hours after trauma. Surgical decompression within the first 4 hours after trauma was not associated with improved neurological outcome compared to treatment between 4 and 24 hours. In a clinical context, this indicates that there is a time frame of at least 1 day in which optimal care is possible.
Most cited references21
- Record: found
- Abstract: found
- Article: not found
Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey?
- Record: found
- Abstract: found
- Article: not found
Timing of decompressive surgery of spinal cord after traumatic spinal cord injury: an evidence-based examination of pre-clinical and clinical studies.
- Record: found
- Abstract: found
- Article: not found