- Record: found
- Abstract: found
- Article: found
Stenting the ductus arteriosus: Case selection, technique and possible complications
Read this article at
Abstract
Ductal stenting is an attractive alternative to conventional shunt surgery in duct dependent congenital heart disease as it avoids thoracotomy and its related problems. With today's generation of coronary stents which have better profile, flexibility and trackability, ductal stenting may be achieved safely and with considerably less difficulty than previously described.
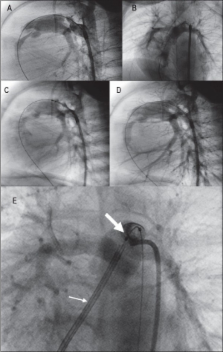
As in Blalock-Taussig (BT) shunt, ductal stenting is indicated mainly in duct-dependent cyanotic lesions chiefly in the neonatal period. Unlike the Patent ductus arteriosus (PDA) as an isolated lesion, the ductus in cyanotic heart disease has a remarkable morphologic variability. The ductus tends to arise more proximally under the aortic arch, giving rise to a vertical ductus or occasionally it may arise from the subclavian artery. It also tends to be long and sometimes very tortuous, rendering stent implantation technically impossible. The ductus in these patients may also insert onto one of the branch pulmonary arteries with some stenosis at the site of insertion. The ductus in Tetralogy of Fallot with pulmonary atresia (TOF-PA) tend to exhibit these morphologic features and to a lesser degree in transposition of great arteries with ventricular septal defect and pulmonary atresia (TGA-VSD-PA) and the more complex forms of univentricular hearts. In the preliminary angiographic evaluation, it is important to delineate these morphologic features as the basis for case selection.
Ductal stenting may be done by the retrograde femoral artery route or the antegrade transvenous route depending on the ductus morphology and the underlying cardiac lesion. The detailed techniques and essential hardware are described. Finally, major potential complications of the procedure are described. Acute stent thrombosis is the most serious and potentially catastrophic. Emergent treatment with thrombolytic therapy and mechanical disruption of thrombus are required. With proper case selection, appropriate technique and the right hardware ductal stenting provides reasonable short-medium term palliation in duct-dependent cyanotic heart disease.
Related collections
Most cited references6
- Record: found
- Abstract: not found
- Article: not found
Angiographic classification of the isolated, persistently patent ductus arteriosus and implications for percutaneous catheter occlusion.
- Record: found
- Abstract: found
- Article: not found
Initial results and medium-term follow-up of stent implantation of patent ductus arteriosus in duct-dependent pulmonary circulation.
- Record: found
- Abstract: found
- Article: not found