- Record: found
- Abstract: found
- Article: found
Sonographically Guided Core Biopsy of the Breast: Comparison of 14-Gauge Automated Gun and 11-Gauge Directional Vacuum-Assisted Biopsy Methods
Read this article at
Abstract
Objective
To compare the outcomes of 14-gauge automated biopsy and 11-gauge vacuum-assisted biopsy for the sonographically guided core biopsies of breast lesions.
Materials and Methods
We retrospectively reviewed all sonographically guided core biopsies performed from January 2002 to February 2004. The sonographically guided core biopsies were performed with using a 14-gauge automated gun on 562 breast lesions or with using an 11-gauge vacuum-assisted device on 417 lesions. The histologic findings were compared with the surgical, imaging and follow-up findings. The histologic underestimation rate, the repeat biopsy rate and the false negative rates were compared between the two groups.
Results
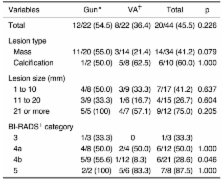
A repeat biopsy was performed on 49 benign lesions because of the core biopsy results of the high-risk lesions (n = 24), the imaging-histologic discordance (n = 5), and the imaging findings showing disease progression (n = 20). The total underestimation rates, according to the biopsy device, were 55% (12/22) for the 14-gauge automated gun biopsies and 36% (8/22) for the 11-gauge vacuum-assisted device ( p = 0.226). The atypical ductal hyperplasia (ADH) underestimation (i.e., atypical ductal hyperplasia at core biopsy and carcinoma at surgery) was 58% (7/12) for the 14-gauge automated gun biopsies and 20% (1/5) for the 11-gauge vacuum-assisted biopsies. The ductal carcinoma in situ (DCIS) underestimation rate (i.e., ductal carcinoma in situ upon core biopsy and invasive carcinoma found at surgery) was 50% (5/10) for the 14-gauge automated gun biopsies and 41% (7/17) for the 11-gauge vacuum-assisted biopsies. The repeat biopsy rates were 6% (33/562) for the 14-gauge automated gun biopsies and 3.5% (16/417) for the 11-gauge vacuum-assisted biopsies. Only 5 (0.5%) of the 979 core biopsies were believed to have missed the malignant lesions. The false-negative rate was 3% (4 of 128 cancers) for the 14-gauge automated gun biopsies and 1% (1 of 69 cancers) for the 11-gauge vacuum-assisted biopsies.
Conclusion
The outcomes of the sonographically guided core biopsies performed with the 11-gauge vacuum-assisted device were better than those outcomes of the biopsies performed with the 14-gauge automated gun in terms of underestimation, rebiopsy and the false negative rate, although these differences were not statistically significant.
Related collections
Most cited references29
- Record: found
- Abstract: found
- Article: not found
Percutaneous large-core breast biopsy: a multi-institutional study.
- Record: found
- Abstract: found
- Article: not found
US-guided automated large-core breast biopsy.
- Record: found
- Abstract: found
- Article: not found