- Record: found
- Abstract: found
- Article: found
Anti-tumour effects of lanreotide for pancreatic and intestinal neuroendocrine tumours: the CLARINET open-label extension study
Abstract
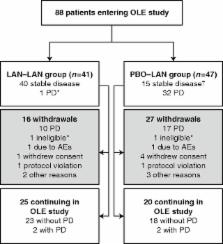
In the CLARINET study, lanreotide Autogel (depot in USA) significantly prolonged progression-free survival (PFS) in patients with metastatic pancreatic/intestinal neuroendocrine tumours (NETs). We report long-term safety and additional efficacy data from the open-label extension (OLE). Patients with metastatic grade 1/2 (Ki-67 ≤10%) non-functioning NET and documented baseline tumour-progression status received lanreotide Autogel 120 mg ( n=101) or placebo ( n=103) for 96 weeks or until death/progressive disease (PD) in CLARINET study. Patients with stable disease (SD) at core study end (lanreotide/placebo) or PD (placebo only) continued or switched to lanreotide in the OLE. In total, 88 patients (previously: lanreotide, n=41; placebo, n=47) participated: 38% had pancreatic, 39% midgut and 23% other/unknown primary tumours. Patients continuing lanreotide reported fewer adverse events (AEs) (all and treatment-related) during OLE than core study. Placebo-to-lanreotide switch patients reported similar AE rates in OLE and core studies, except more diarrhoea was considered treatment-related in OLE (overall diarrhoea unchanged). Median lanreotide PFS (core study randomisation to PD in core/OLE; n=101) was 32.8 months (95% CI: 30.9, 68.0). A sensitivity analysis, addressing potential selection bias by assuming that patients with SD on lanreotide in the core study and not entering the OLE ( n=13) had PD 24 weeks after last core assessment, found median PFS remaining consistent: 30.8 months (95% CI: 30.0, 31.3). Median time to further PD after placebo-to-lanreotide switch ( n=32) was 14.0 months (10.1; not reached). This OLE study suggests long-term treatment with lanreotide Autogel 120 mg maintained favourable safety/tolerability. CLARINET OLE data also provide new evidence of lanreotide anti-tumour benefits in indolent and progressive pancreatic/intestinal NETs.
Related collections
Most cited references8
- Record: found
- Abstract: found
- Article: not found
Sunitinib malate for the treatment of pancreatic neuroendocrine tumors.
- Record: found
- Abstract: found
- Article: not found
Lanreotide in metastatic enteropancreatic neuroendocrine tumors.
- Record: found
- Abstract: found
- Article: found
Rapid and Sustained Relief from the Symptoms of Carcinoid Syndrome: Results from an Open 6-Month Study of the 28-Day Prolonged-Release Formulation of Lanreotide
Author and article information
Journal
Affiliations
Author notes
Article
ERC150490
 This work is licensed under a
Creative Commons Attribution 3.0 Unported License
This work is licensed under a
Creative Commons Attribution 3.0 Unported License