
Introduction
Cardiac myxomas are the commonest primary cardiac tumors, with an extremely low incidence of between 0.0017 and 0.19% [1]. Although myxomas are histologically benign, fatal events can occasionally occur in the case of systemic and cerebral embolism. The clinical features differ depending on the size, location, structure, mobility, and fragility of the mass, and only about one-fifth of myxomas originate from the right chambers of the heart [1]. Herein we present a rare case of a giant right atrial myxoma with blood supply from the left and right coronary arteries and the multimodality imaging features.
Case Presentation
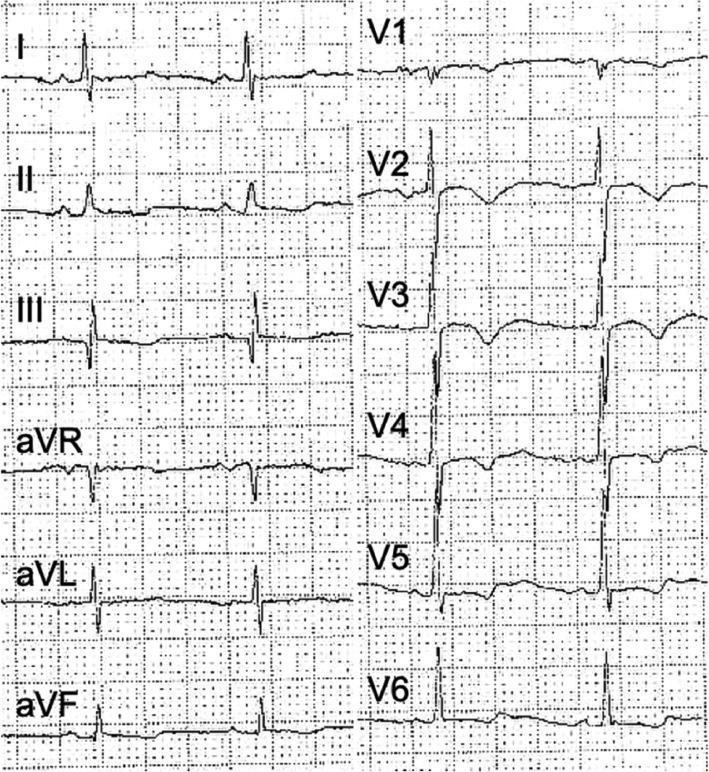
A 60-year-old woman was admitted because of recurrent attacks of chest tightness and shortness of breath during the previous 6 months especially after exercise. No remarkable abnormality was found on physical examination. About 3 months before her admission, a routine 12-lead electrocardiogram (Figure 1) and transthoracic echocardiography (Figure 2A) were performed after she had experienced a recurrent episode of chest tightness, and a giant mass in the right atrium was detected by echocardiography. To clarify the nature of the huge mass, [18F]fluorodeoxyglucose PET/CT was performed, and the low-density mass in delayed imaging with the standard uptake value of 2.3 for the radioactive concentration was suggestive of imaging features of myxoma (Figure 3A and B). Because of the ischemic characteristics of the electrocardiogram (T-wave inversion in precordial leads, nonspecific ST-T abnormality shown in Figure 1) and the patient’s age and presenting symptoms, preoperative selective coronary angiography was performed to assess the extent and severity of coronary stenosis, and showed no significant stenosis in the coronary arteries, but a strongly neovascularized right atrial mass that was supplied by two feeding vessels with multiple branches from the left and right coronary arteries (Figure 4, Videos 1 and 2, Videos 1 and 2 may be downloaded at the following links: Video 1: http://cvia-journal.org/wp-content/uploads/2020/01/CVIA_196_VIDEO_1.avi and Video 2: http://cvia-journal.org/wp-content/uploads/2020/01/CVIA_196_VIDEO_2.avi). The myxoma was successfully excised with open heart surgery. Pathological analysis (Figure 3C) confirmed the diagnosis of atrial myxoma. Echocardiography performed 2 months and 3 years after surgery showed no evidence of myxoma recurrence (Figure 2B and C).
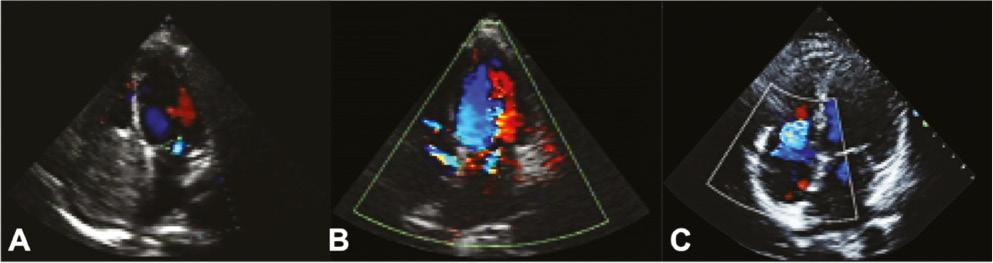
Transthoracic echocardiography showing a mass of 62.5 mm×57.3 mm nearly filling the whole right atrium (A) and the return to normal size of the enlarged right atrium at 2 months (B) and 3 years (C) after surgery.

Preoperative [18F]fluorodeoxyglucose PET/CT (A and B) suggesting a low-density mass in delayed imaging with the standard uptake value of 2.3 for the radioactive concentration and punctate calcification in the mass. Hematoxylin-eosin staining (C) of the mass confirmed myxoma rich in blood vessels.

Discussion
Cardiac myxomas, the commonest primary benign cardiac tumors, are extremely rare, with an incidence ranging from 0.0017 to 0.19% and only 15–20% of them originating from the right chambers of the heart [1]. In the present case, we report a rare giant right atrial myxoma nearly filling the whole right atrium with left and right coronary artery blood supply.
The clinical diagnosis of cardiac myxoma is often challenging because of its nonspecific clinical and radiological features, which may even mimic endocarditis or cancer [1]. Typical symptoms and electrocardiogram features of myocardial ischemia of the patient should be due to the coronary steal phenomenon caused by neovascularization of the cardiac myxoma and intracardiac obstruction, which may cause right ventricular hypertrophy, pulmonary hypertension, right ventricular failure, hepatomegaly, etc.
Two-dimensional transthoracic echocardiography, which can accurately define the location, size, structure, and mobility of the mass, is the most preferred, commonly used, and cost-effective imaging technique to detect cardiac myxomas [2]. However, differential diagnosis between cardiac myxoma and thrombus may be a great challenge as the attachment point is difficult to determine, especially when the mass is so big that it fills the whole chamber of the heart. Two-dimensional transthoracic echocardiography may provide more accurate information on the mass for the differential diagnosis.
[18F]Fluorodeoxyglucose PET/CT is usually performed to rule out cardiac malignancies and assess systemic metastasis [3]. However, it may make the diagnosis much more difficult when no [18F]fluorodeoxyglucose uptake is seen. In the present case, the standard uptake value of the radioactive concentration was low, but a clear outline and the attachment point were seen, which may facilitate exclusion of a diagnosis of cardiac thrombus.
The indication for routine selective coronary angiography before open heart surgery is still controversial [4]. The main reasons for this invasive examination before surgery are (1) ruling out undiagnosed significant coronary artery disease especially for patients with high risk factors for coronary artery disease, (2) assessing the extent and severity of coronary stenosis for patients with diagnosed coronary artery disease to determine the optimal operating time since serious coronary stenosis may be first treated before surgery, and (3) assessing the vascular supply of the myxoma, which may change the approach, preferred methods, and blood-ordering schedule for surgery. Tumor neovascularization, which was visible in up to 80% of myxoma cases [5, 6], is not specific for cardiac myxomas. Left-sided and right-sided myxomas were mostly supplied from the left circumflex artery and the right coronary artery, respectively [7]. Neovascularization originating from both the right coronary artery and the left circumflex artery was reported in a left atrial myxoma [8], but no similar case in a right atrial myxoma has been reported to our knowledge.
Other imaging techniques [9], such as CT and cardiovascular MRI, could provide accurate information to assist the diagnosis of cardiac myxomas, but for one specific individual it is essential to diagnose myxomas with fewer examinations.