- Record: found
- Abstract: found
- Article: found
Non-pharmacological Treatment for Chronic Pain in US Veterans Treated Within the Veterans Health Administration: Implications for Expansion in US Healthcare Systems
Read this article at
Abstract
Background
Consensus guidelines recommend multimodal chronic pain treatment with increased use of non-pharmacological treatment modalities (NPM), including as first-line therapies. However, with many barriers to NPM uptake in US healthcare systems, NPM use may vary across medical care settings. Military veterans are disproportionately affected by chronic pain. Many veterans receive treatment through the Veterans Health Administration (VHA), an integrated healthcare system in which specific policies promote NPM use.
Objective
To examine whether veterans with chronic pain who utilize VHA healthcare were more likely to use NPM than veterans who do not utilize VHA healthcare.
Main Measures
In the 2019 National Health Interview Survey, veterans were assessed for VHA treatment, chronic pain (i.e., past 3-month daily or almost daily pain), symptoms of depression and anxiety, substance use, and NPM (i.e., physical therapy, chiropractic/spinal manipulation, massage, psychotherapy, educational class/workshop, peer support groups, or yoga/tai chi).
Key Results
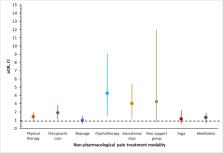
Chronic pain (45.2% vs. 26.8%) and NPM use (49.8% vs. 39.4%) were more prevalent among VHA patients than non-VHA veterans. After adjusting for sociodemographic characteristics, psychiatric symptoms, physical health indicators, and use of cigarettes or prescription opioids, VHA patients were more likely than non-VHA veterans to use any NPM (adjusted odds ratio [aOR] = 1.52, 95% CI: 1.07–2.16) and multimodal NPM (aOR = 1.80, 95% CI: 1.12–2.87) than no NPM. Among veterans with chronic pain, VHA patients were more likely to use chiropractic care (aOR = 1.90, 95% CI = 1.12–3.22), educational class/workshop (aOR = 3.02, 95% CI = 1.35–6.73), or psychotherapy (aOR = 4.28, 95% CI = 1.69–10.87).
Conclusions
Among veterans with chronic pain, past-year VHA use was associated with greater likelihood of receiving NPM. These findings may suggest that the VHA is an important resource and possible facilitator of NPM. VHA policies may offer guidance for expanding use of NPM in other integrated US healthcare systems.
Related collections
Most cited references66
- Record: found
- Abstract: found
- Article: not found
A brief measure for assessing generalized anxiety disorder: the GAD-7.
- Record: found
- Abstract: found
- Article: not found
The PHQ-8 as a measure of current depression in the general population.
- Record: found
- Abstract: found
- Article: not found