- Record: found
- Abstract: found
- Article: found
Fatty tumors of the retroperitoneum: Lipoma or well-differentiated liposarcoma. About a case of a giant retroperitoneal liposarcoma
case-report
Mokhtar bibi
a
,
∗ ,
Sami Ben Rhouma
a ,
Yassine Ouanes
a ,
Beya Chelly
b ,
Zinet Ghorbel
b ,
Ahmed Sellami
a ,
Asma Souid
c ,
Seif Boukriba
c ,
Mohamed Ali Ben Chehida
a ,
Yassine Nouira
a
04 September 2018
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Introduction
Fatty tumors of the retroperitoneum are rare and represent a real dilemma for urologist.
Distinguishing between liposarcoma whish is a poor prognosis tumor and lipoma which
is a benign tumor is sometimes difficult. We report the case of a 26 year-old, women
presenting a giant fatty retroperitoneal mass measuring 17 × 10 cm.
Through this case we report the management of the patient and we discuss diagnostic
difficulties and treatment.
Case
A 26- year-old woman was referred to our center with a giant retroperitoneal mass.
The patient complained about abdominal swelling and recurrent episodes of abdominal
pain. Computed Tomography (CT) scan of the abdomen and pelvis showed a mass arising
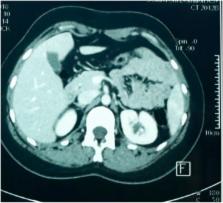
in the retroperitoneum. It was a homogenous hypodense mass surrounded by a thin capsule,
well limited, measuring 10 × 8 × 17 cm and containing few thin septa. This mass was
diagnosed as a lipoma by radiologist (Fig. 1A). The mass was in contact with the inferior
vena cava, under the right kidney which was compressed on the posterior abdominal
wall and represses the peritoneal containing to the left part of abdomen (Fig. 1B).
No significant contrast enhancement was detected. We considered the mass resectable
however very close to the right kidney. An open biopsy and intraoperative judgment
helped the decision of complete resection of the tumor rather than en-bloc removal
of the mass and right kidney.
Fig. 1
A: Contrast enhanced CT scan in the axial plane showing a giant homogenous mass, mainly
consisting of fat tissue surrounded by a thin capsule arising in the retroperitoneum
pushing the right kidney to the posterior wall (*). B: Contrast enhanced CT scan in
the coronal plane showing a 17 cm retroperitoneal mass repressing organs to the left
and lower part of the abdomen.
Fig. 1
The patient was operated through a Kocher incision. We found a giant clearly encapsulated
fatty tumor deriving from the right retroperitoneal fatty tissue. An open biopsy of
3 cm in size was performed. Frozen section examination concluded to a retroperitoneal
adipocytic tumor without cytologic atypia. The mass was completely extirpated without
resection of adjacent tissue or organs. The patient was discharged on the fourth postoperative
day without complications. The final histopathological report showed a well-differentiated
liposarcoma of the retroperitoneum with mature adipocytic proliferation and presence
of atypical, hyperchromatic stromal cells with lipoblasts (Fig. 2A and B). At 1 year
post-surgery, there was no evidence of recurrence on different CT scans (Fig. 3).
Fig. 2
A: Histological examination showed a mature adipocytic proliferation with variation
in cell size. (Hematoxylin-Eosin, x 20). B: Histological examination showed presence
of atypical, hyperchromatic stromal cells with a varying number of lipoblasts. (Hematoxylin-Eosin,
x 40).
Fig. 2
Fig. 3
Contrast enhanced CT scan in the axial plane after 1 year of follow up, showing no
signs of recurrence.
Fig. 3
Discussion
Liposarcomas represent the most common type of sarcoma arising in the retroperitoneum.
The rarity of retroperitoneal liposarcomas and the variety of histologic subtypes
make it difficult to understand and treat this neoplasm.
1
The distinction between lipoma and well-differentiated liposarcoma is a frequent diagnostic
dilemma. Computed tomography (CT) imaging features that suggest malignancy include
large lesion size, presence of thick septa, presence of nodular and/or globular or
non adipose masslike areas, and decreased percentage of fat composition.
2
Histopathology is fundamental for the diagnostic workup of lipomatous tumors. It can
show fibrillar fibrous septa containing enlarged hyperchromatic cells and rare lipoblasts.
However, there are some lipoma-like well differentiated liposarcoma that may be extremely
difficult to distinguish confidently from lipoma due to their extreme paucity of hyperchromatic
cells and lipoblasts.
3
In that case an immunohistochemical panel composed of MDM2 and CDK4 is recommended.
Fluorescence in situ hybridization (FISH) for MDM2 amplification can be useful to
discriminate lipomas from atypical lipomatous tumor and well-differentiated Liposarcomas.
4
In our case, MDM2 and CDK4 are unfortunately unavailable. Surgery is the mainstay
of treatment of non-metastatic retroperitoneal lipomatous tumors. Whenever is possible,
a macroscopically complete resection should be aimed at, often requiring en-bloc removal
of adjacent structures.
5
In case of unresectability or patients with hematogenous metastases a biopsy should
be reserved. Tissue may be obtained through fine-needle aspiration or core-needle
biopsy. Percutaneous biopsies are reliable and safe. However, percutaneous techniques
have a low subtype specific diagnostic in liposarcoma. In our case, CT scan images
and frozen section examination concluded to a retroperitoneal lipoma however final
histological examination showed presence of atypical, hyperchromatic stromal cells
confirming the diagnosis of well-differentiated liposarcoma. The current guidelines
from the National Comprehensive Cancer Network for the surveillance of retroperitoneal
sarcomas recommend that patients with low-grade tumors who have been successfully
resected should have a follow-up physical examination with imaging (chest/abdominal/pelvic
CT) every 3–6 months for 2–3 years, then annually.
Conclusion
The distinction of lipoma-like well-differentiated liposarcoma from lipoma is difficult.
The large lesion size, presence of thick septa, presence of nodular areas on CT scan,
intraoperative judgment and mature adipose tissue on histology could make the diagnosis.
Molecular testing could be useful in the differential diagnosis of lipomatous tumors.
The resection should be complete with a strict follow up.
Conflicts of interest
None for all authors.
Funding
This research did not receive any specific grant from funding agencies in the public,
commercial, or not-for-profit sectors.
Related collections
Most cited references3
- Record: found
- Abstract: found
- Article: not found
Well-differentiated liposarcoma. The Mayo Clinic experience with 58 cases.
Brandon Lucas, M G Rock, Oliver A. Nascimento … (1994)
- Record: found
- Abstract: found
- Article: not found
MDM2 Amplification in Problematic Lipomatous Tumors: Analysis of FISH Testing Criteria.
Mark A Edgar, Sharon Weiss, Anthony P Martinez … (2015)
- Record: found
- Abstract: found
- Article: not found
Retroperitoneal lipomatous tumors without cytologic atypia: are they lipomas? A clinicopathologic and molecular study of 19 cases.
Michele Erickson-Johnson, David Rubin, R Macarenco … (2009)