- Record: found
- Abstract: found
- Article: found
Cemented vs. cementless fixation in primary total knee arthroplasty: a systematic review and meta-analysis
Read this article at
Abstract
-
Over 100,000 total knee replacements (TKRs) are carried out in the UK annually, with cemented fixation accounting for approximately 95% of all primary TKRs. In Australia, 68.1% of all primary TKRs use cemented fixation, and only 10.9% use cementless fixation. However, there has been a renewed interest in cementless fixation as a result of improvements in implant design and manufacturing technology.
-
This meta-analysis aimed to compare the outcomes of cemented and cementless fixation in primary TKR. Outcome measures included the revision rate and patient-reported functional scores.
-
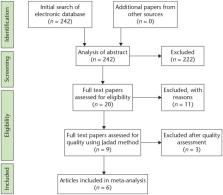
MEDLINE and EMBASE were searched from the earliest available date to November 2018 for randomized controlled trials of primary TKAs comparing cemented versus cementless fixation outcomes.
-
Six studies met our inclusion criteria and were analysed. A total of 755 knees were included; 356 knees underwent cemented fixation, 399 underwent cementless fixation. They were followed up for an average of 8.4 years (range: 2.0 to 16.6).
-
This study found no significant difference in revision rates and knee function in cemented versus cementless TKR at up to 16.6-year follow-up.
Cite this article: EFORT Open Rev 2020;5:793-798. DOI: 10.1302/2058-5241.5.200030
Related collections
Most cited references39
- Record: found
- Abstract: found
- Article: not found
Assessing the quality of reports of randomized clinical trials: is blinding necessary?
- Record: found
- Abstract: found
- Article: not found
The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study.
- Record: found
- Abstract: found
- Article: not found