
- Record: found
- Abstract: found
- Article: found
Areas of delay related to prolonged length of stay in an emergency department of an academic hospital in South Africa
Read this article at
Abstract
Introduction
Globally, length of stay of patients in emergency departments remains a challenge. Remaining in the emergency department for >12 h increases health care costs, morbidity and mortality rates and leads to crowding and lower patient satisfaction.
The aim of this research was to describe the areas of delay related to prolonged length of stay in the emergency department of an academic hospital.
Methods
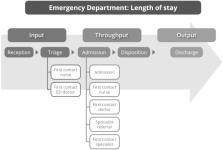
A quantitative retrospective study was done. The Input-Throughput-Output model was used to identify the areas of patients' journey through the emergency department. The possible areas of delay where then described. Using systematic sampling, a total of 100 patient files managed in an emergency department of an academic hospital in South Africa were audited over a period of 3 months. Descriptive statistics and regression analysis was used to analyse data.
Results
The mean length of stay of patients in the emergency department was 73 h 49 min. The length of stay per phase was: input (3 h 17 min), throughput (16 h 25 min) and output (54 h 7 min). A strong significant relationship found between the length of stay and the time taken between disposition decision (throughput phase) disposition decision to admission or discharge of patients from the ED (output phase) (p < 0.05).
Related collections
Most cited references51
- Record: found
- Abstract: found
- Article: not found
A conceptual model of emergency department crowding.

- Record: found
- Abstract: found
- Article: found
Implementation and evaluation of a rural community-based pediatric hearing screening program integrating in-person and tele-diagnostic auditory brainstem response (ABR)
- Record: found
- Abstract: found
- Article: not found