- Record: found
- Abstract: found
- Article: found
Which is your diagnosis? Translated title: Qual o seu diagnóstico?
case-report
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
A 26-year-old male patient, drugs user, presenting with dry cough and fever for two
weeks.
The patient has a diagnosis of acquired immunodeficiency syndrome (AIDS), with poor
adherence to the treatment. His CD4 count was 20 cells/mm3 and the viral load
was 495,208 cps/ml. Chest radiography demonstrated opacity in the right upper lobe
of the
lung. Chest computed tomography was performed (Figure
1).
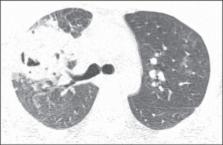
Figure 1
Computed tomography with window for pulmonary parenchyma. Section at the level of
the
carina
Image description
Figure 1. Chest computed tomography
shows cavitated consolidation in the right upper lobe of the lung. Also, one observes
small nodules and ground glass opacities adjacent to the described image as well as
in
the contralateral lung.
Diagnosis:
Rhodococcus equi pneumonia in an AIDS patient.
Open biopsy was performed and culture demonstrated bacterial growth.
COMMENTS
R. equi is a Gram-positive cocci that commonly causes infection in
horses and other animals. R. equi infection is rarely found in
humans(1), affecting
particularly individuals at advanced degree of immunodeficiency. About 80% of cases
occur in AIDS patients, most of times in those presenting CD4 lymphocyte count lower
than 200 cell/mm3(2,3).
In humans, the main infection site is the lung(1). The most frequent clinical presentation
is a slow-growing
pneumonic process, with cough, fever and constitutional symptoms. R.
equi represents a frequent cause of bacteremia and extra-pulmonary signs may
be found. The etiological agent can be easily isolated from the sites of
infection(2).
The main pattern of lung involvement is that of masses with heterogeneous contrast
impregnation or foci of pulmonary consolidation intermingled with air bronchograms,
either with or without cavitated lesions. Although cavitation may be not present at
the
moment of the diagnosis, it ends up developing along the disease progression(4). Other
findings include ground glass
opacities, air-space nodules, small nodules with predominantly centrilobular
distribution and the tree-in-bud pattern predominantly located around consolidations.
Probably, such findings represent bronchogenic dissemination of the infection.
Mediastinal lymph nodes enlargement may be present(1,2,4-8).
The typical histopathological finding of R. equi infection corresponds
to necrotizing cavitation or soft tissue mass composed of a dense histiocytic infiltrate
with abundant eosinophilic granular cytoplasm. Polymorphonuclear leukocytes are numerous
in disseminated microabscesses. Periodic acid Schiff staining demonstrates highly
positive histiocytes similar to those observed in Whipple's disease. Gram-positive
cocci
are easy demonstrated at Gram tissue stain. Pulmonary malakoplakia is another finding
described in R. equi infection(9).
The differential diagnoses for pulmonary R. equi infection in AIDS
patients include cavitated infections (tuberculosis, nocardiosis, fungal diseases,
lung
abscess), lung neoplasms, and more remotely Pneumocystis jiroveci
pneumonia (7,10,11). Micobacterium
tuberculosis infection, however, is the main differential diagnosis to be considered
for
patients with R. equi pneumonia, since both bacilli are alcohol-acid
resistant.
The diagnosis of disease activity in patients with pulmonary tuberculosis depends
on
multiple factors, namely, clinical signs, physical examination, tuberculin test results
and, mainly, detection of the bacillus in sputum, bronchoalveolar lavage, transtracheal
aspirate or in lung biopsy specimen, being reinforced by other factors such as
sequential alterations at serial chest radiography and previous history of
antituberculosis therapy. However, the diagnosis may be difficult considering the
facts
that sputum bacilloscopy may be negative in 21-66% of cases and it may take up to
six
weeks for a bacillus colony to grow in a culture, and that findings at chest radiography
are frequently classified as indeterminate(12-14).
High-resolution computed tomography (HRCT) has shown to be superior to plain radiography
in the detection and evaluation of extent of parenchymal alterations, considering
that
because of its effectiveness in the evaluation of the secondary lung lobe, it allows
for
a better characterization of pathological pulmonary processes. A recent series of
studies published by Brazilian authors(15-23) corroborates such
assertion. Thus, HRCT plays an extremely relevant role in the diagnosis of pulmonary
tuberculosis.
HRCT findings in patients with post-primary tuberculosis include centrilobular nodules,
air space nodules, nodular opacities, tree-in-bud pattern, miliary nodules,
consolidations, cavitations, bronchial walls thickening, tuberculomas, calcifications,
parenchymal bands, interlobular septal thickening, ground glass opacities,
pericicatricial emphysema and fibrotic alterations(12,13,24-32). Other
manifestations recently described include reversed halo sign and clusters of
micronodules, either with or without confluence(33-35). Most of such findings
can also be observed in patients with R. equi pneumonia.
In conclusion, R. equi infection should be considered in the
differential diagnosis of cavitated consolidations in AIDS patients, with a particular
difficult differentiation from lesions caused by tuberculosis.
Related collections
Most cited references107
- Record: found
- Abstract: found
- Article: not found
Pulmonary tuberculosis: CT findings--early active disease and sequential change with antituberculous therapy.
Jongmin Lee, H Itoh, Y Shim … (1993)
- Record: found
- Abstract: found
- Article: not found
Pulmonary tuberculosis: up-to-date imaging and management.
- Record: found
- Abstract: found
- Article: not found
High resolution computed tomographic findings in pulmonary tuberculosis.
Eyup Ucan, E Osma, Osman Hatipoglu … (1996)