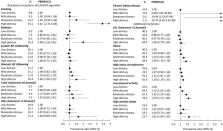
People who experience psychological distress have an elevated risk of incident cardiovascular disease (CVD). However, the extent to which traditional CVD prevention strategies could be used to reduce the CVD burden in this group is unclear because population-level data on CVD risk profiles and appropriate management of risk in relation to distress are currently not available. The aim of this study was to use nationally representative data to quantify variation in CVD risk and appropriate management of risk according to level of psychological distress in the Australian population. Data were from 2,618 participants aged 45–74 years without prior CVD who participated in the 2011-12 Australian Health Survey, a cross-sectional and nationally representative study of Australian adults. Age-and sex-adjusted prevalence of 5-year absolute risk of primary CVD (low <10%, moderate 10–15%, or high >15%), CVD risk factors, blood-pressure, and cholesterol assessments, and appropriate treatment (combined blood pressure- and lipid-lowering medication) if at high primary risk, were estimated. Prevalence ratios (PR) quantified variation in these outcomes in relation to low (Kessler-10 score: 10-<12), mild (12-<16), moderate (16-<22) and high (22–50) psychological distress, after adjusting for sociodemographic characteristics. The prevalence of high absolute risk of primary CVD for low, mild, moderate and high distress was 10.9, 12.3, 11.4, and 18.6%, respectively, and was significantly higher among participants with high compared to low distress (adjusted PR:1.62, 95%CI:1.04–2.52). The prevalence of CVD risk factors was generally higher in those with higher psychological distress. Blood pressure and cholesterol assessments were reported by the majority of participants (>85%) but treatment of high absolute risk was low (<30%), and neither were related to psychological distress. Our findings confirm the importance of recognizing people who experience psychological distress as a high risk group and suggest that at least part of the excess burden of primary CVD events among people with high psychological distress could be reduced with an absolute risk approach to assessment and improved management of high primary CVD risk.