
- Record: found
- Abstract: found
- Article: found
Contrasting Perspectives of Anesthesiologists and Gastroenterologists on the Optimal Time Interval between Bowel Preparation and Endoscopic Sedation
Read this article at
Abstract
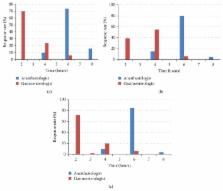
Background. The optimal time interval between the last ingestion of bowel prep and sedation for colonoscopy remains controversial, despite guidelines that sedation can be administered 2 hours after consumption of clear liquids. Objective. To determine current practice patterns among anesthesiologists and gastroenterologists regarding the optimal time interval for sedation after last ingestion of bowel prep and to understand the rationale underlying their beliefs. Design. Questionnaire survey of anesthesiologists and gastroenterologists in the USA. The questions were focused on the preferred time interval of endoscopy after a polyethylene glycol based preparation in routine cases and select conditions. Results. Responses were received from 109 anesthesiologists and 112 gastroenterologists. 96% of anesthesiologists recommended waiting longer than 2 hours until sedation, in contrast to only 26% of gastroenterologists. The main reason for waiting >2 hours was that PEG was not considered a clear liquid. Most anesthesiologists, but not gastroenterologists, waited longer in patients with history of diabetes or reflux. Conclusions. Anesthesiologists and gastroenterologists do not agree on the optimal interval for sedation after last drink of bowel prep. Most anesthesiologists prefer to wait longer than the recommended 2 hours for clear liquids. The data suggest a need for clearer guidelines on this issue.
Related collections
Most cited references22
- Record: found
- Abstract: not found
- Article: not found
Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters.
- Record: found
- Abstract: found
- Article: not found
Risk of gastroparesis in subjects with type 1 and 2 diabetes in the general population.
- Record: found
- Abstract: found
- Article: not found