- Record: found
- Abstract: found
- Article: found
Study design of Real World Evidence for Treatment of Hyperkalemia in the Emergency Department (REVEAL-ED): a multicenter, prospective, observational study
Read this article at
Abstract
Objective
Hyperkalemia affects up to 10% of hospitalized patients and, if left untreated, can lead to serious cardiac arrhythmias or death. Although hyperkalemia is frequently encountered in the emergency department (ED), and is potentially life-threatening, standard of care for the treatment is poorly defined, with little supporting evidence. The main objectives of this observational study are to define the overall burden of hyperkalemia in the ED setting, describe its causes, the variability in treatment patterns and characterize the effectiveness and safety of ED standard of care therapies used in the United States.
Methods
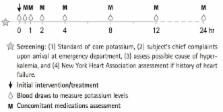
This is an observational study evaluating the management of hyperkalemia in the ED. Two hundred and three patients who presented to the ED with a potassium value ≥5.5 mmol/L were enrolled in the study at 14 sites across the United States. Patients were treated per standard of care practices at the discretion of the patient’s physician. In patients who received a treatment for hyperkalemia, blood samples were drawn at pre-specified time points and serum potassium values were recorded. The change in potassium over 4 hours and the adverse events after standard of care treatment were analyzed.
Results and Conclusion
This article describes the background, rationale, study design, and methodology of the REVEAL-ED (Real World Evidence for Treatment of Hyperkalemia in the Emergency Department) trial, a multicenter, prospective, observational study evaluating contemporary management of patients admitted to the ED with hyperkalemia.
Related collections
Most cited references13
- Record: found
- Abstract: found
- Article: not found
Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study.
- Record: found
- Abstract: found
- Article: not found
The frequency of hyperkalemia and its significance in chronic kidney disease.
- Record: found
- Abstract: found
- Article: not found