- Record: found
- Abstract: found
- Article: found
Diagnosis and treatment of epididymal tuberculosis: a review of 47 cases
Read this article at
Abstract
Objective
To analyze the clinical manifestations, diagnosis and treatment outcomes in a series of patients with epididymal tuberculosis.
Methods
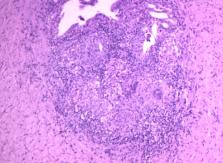
This study is a retrospective data analysis of 47 cases of histologically-confirmed epididymal tuberculosis in patients treated at our hospital from November 2012 to December 2018.
Results
The average age of the patients was approximately 42 years. The epididymal lesion location was left-sided in 15 patients (31.9%), right-sided in 22 patients (46.8%) and bilateral in 10 patients (21.3%). The main symptoms were painless swelling of the scrotum in 21 cases (44.7%) and scrotal drop pain in 21 cases (44.7%). Scrotal physical examination revealed epididymal beaded enlargement in 12 patients (25.5%), testicular mass in one patient (2.1%), scrotal tenderness alone in seven patients (14.9%), ill-defined epididymal-testicular border in 21 patients (44.7%) and sinus formation in six patients (12.8%). After 2–4 weeks of anti-tuberculosis chemotherapy, the patients underwent a surgical procedure. We found that 10 (83.3%) of the 12 patients whose main symptom was epididymal beaded enlargement underwent simple epididymal surgery. Of the 21 patients whose main clinical manifestation was ill-defined testis-epididymis demarcation, 16 (72.2%) underwent epididymis-testicular surgery. All patients underwent postoperative chemotherapy for 3–6 months. Postoperative follow-up showed good response to treatment.
Conclusion
It is difficult to diagnose early-stage epididymal tuberculosis. Epididymal tuberculosis is likely to have invaded surrounding tissues when signs such as epididymal beaded changes and ill-defined epididymis-testis border are present. Surgical treatment combined with preoperative and postoperative chemotherapy is an effective approach to treating this condition.
Related collections
Most cited references16
- Record: found
- Abstract: found
- Article: not found
Therapeutic drug monitoring in the treatment of tuberculosis: an update.
- Record: found
- Abstract: found
- Article: not found