- Record: found
- Abstract: found
- Article: found
Factors Associated With Opioid Overdose After an Initial Opioid Prescription
Read this article at
Abstract
This cohort study investigates patient- and prescription-related factors associated with opioid-related fatal or nonfatal overdose among opioid-naive individuals receiving an initial opioid prescription.
Key Points
Question
What factors are associated with an increased risk for opioid overdose after the initial opioid prescription to a previously opioid-naive individual?
Findings
In this cohort study of 236 921 individuals who received a first opioid prescription, 667 experienced an incident opioid overdose. Patient risk factors included being aged 75 years or older, being male, receiving Medicaid or Medicare Advantage coverage, having a comorbid substance use disorder or depression, and having medical comorbidities. Prescription-related risk factors included an initial prescription of oxycodone or tramadol, concurrent use of benzodiazepines, and filling opioid prescriptions from 3 or more pharmacies.
Meaning
Findings from this study suggest that several patient- and prescription-related risk factors are associated with opioid overdose; prescribers, researchers, policy makers, and insurers can apply this information to guide opioid counseling and monitoring, develop clinical decision-making tools, and provide additional opioid prevention and treatment resources to individuals who are at greatest risk for opioid overdose.
Abstract
Objective
To assess the patient factors and early time-varying prescription-related factors associated with opioid-related fatal or nonfatal overdose.
Design, Setting, and Participants
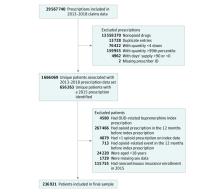
This cohort study evaluated opioid-naive adult patients in Oregon using data from the Oregon Comprehensive Opioid Risk Registry, which links all payer claims data to other health data sets in the state of Oregon. The observational, population-based sample filled a first (index) opioid prescription in 2015 and was followed up until December 31, 2018. Data analyses were performed from March 1, 2020, to June 15, 2021.
Main Outcomes and Measures
The outcome was an overdose event. The sample was followed up to identify fatal or nonfatal opioid overdoses. Patient and prescription characteristics were identified. Prescription characteristics in the first 6 months after the index prescription were modeled as cumulative, time-dependent measures that were updated monthly through the sixth month of follow-up. A time-dependent Cox proportional hazards regression model was used to assess patient and prescription characteristics that were associated with an increased risk for overdose events.
Results
The cohort comprised 236 921 patients (133 839 women [56.5%]), of whom 667 (0.3%) experienced opioid overdose. Risk of overdose was highest among individuals 75 years or older (adjusted hazard ratio [aHR], 3.22; 95% CI, 1.94-5.36) compared with those aged 35 to 44 years; men (aHR, 1.29; 95% CI, 1.10-1.51); those who were dually eligible for Medicaid and Medicare Advantage (aHR, 4.37; 95% CI, 3.09-6.18), had Medicaid (aHR, 3.77; 95% CI, 2.97-4.80), or had Medicare Advantage (aHR, 2.18; 95% CI, 1.44-3.31) compared with those with commercial insurance; those with comorbid substance use disorder (aHR, 2.74; 95% CI, 2.15-3.50), with depression (aHR, 1.26; 95% CI, 1.03-1.55), or with 1 to 2 comorbidities (aHR, 1.32; 95% CI, 1.08-1.62) or 3 or more comorbidities (aHR, 1.90; 95% CI, 1.42-2.53) compared with none. Patients were at an increased overdose risk if they filled oxycodone (aHR, 1.70; 95% CI, 1.04-2.77) or tramadol (aHR, 2.80; 95% CI, 1.34-5.84) compared with codeine; used benzodiazepines (aHR, 1.06; 95% CI, 1.01-1.11); used concurrent opioids and benzodiazepines (aHR, 2.11; 95% CI, 1.70-2.62); or filled opioids from 3 or more pharmacies over 6 months (aHR, 1.38; 95% CI, 1.09-1.75).
Conclusions and Relevance
This cohort study used a comprehensive data set to identify patient and prescription-related risk factors that were associated with opioid overdose. These findings may guide opioid counseling and monitoring, the development of clinical decision-making tools, and opioid prevention and treatment resources for individuals who are at greatest risk for opioid overdose.
Related collections
Most cited references41
- Record: found
- Abstract: found
- Article: not found
Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data.
- Record: found
- Abstract: found
- Article: not found
CDC Guideline for Prescribing Opioids for Chronic Pain--United States, 2016.
- Record: found
- Abstract: not found
- Article: not found