- Record: found
- Abstract: found
- Article: found
Parent–child agreement on health-related quality of life (HRQOL): a longitudinal study
Read this article at
Abstract
Background
Few studies have evaluated changes on parent–child agreement in HRQOL over time. The objectives of the study were to assess parent–child agreement on child’s HRQOL in a 3-year longitudinal study, and to identify factors associated with possible disagreement.
Methods
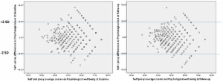
A sample of Spanish children/adolescents aged 8–18 years and their parents both completed the KIDSCREEN-27 questionnaire. Data on age, gender, family socioeconomic status (SES), and mental health (Strengths and Difficulties Questionnaire, SDQ) was also collected at baseline (2003), and again after 3 years (2006). Changes in family composition were collected at follow-up. Agreement was assessed through intraclass correlation coefficient (ICC), and Bland and Altman plots. Generalizing Estimating Equation (GEE) models were built to analyze factors associated with parent–child disagreement.
Results
A total of 418 parent–child pairs were analyzed. At baseline the level of agreement on HRQOL was low to moderate and it was related to the level of HRQOL reported. Physical well-being at baseline showed the highest level of parent–child agreement (ICC=0.59; 0.53-0.65) while less “observable” dimensions presented lower levels of agreement, (i.e. Psychological well-being: ICC= 0.46; 0.38-0.53). Agreement parent–child was lower at follow-up. Some interactions were found between rater and child’s age; with increasing age, child scored lower than parents on Parents relationships and Autonomy (Beta [B] -0.47; -0.71 / -0.23) and the KIDSCREEN-10 (−0.49; -0.73 /-0.25).
Related collections
Most cited references28
- Record: found
- Abstract: found
- Article: not found
Statistical methods for assessing agreement between two methods of clinical measurement.
- Record: found
- Abstract: found
- Article: not found
Integrating response shift into health-related quality of life research: a theoretical model.
- Record: found
- Abstract: found
- Article: not found