- Record: found
- Abstract: found
- Article: found
Epicardial macroreentrant atrial tachycardia involving a large left atrial roof diverticulum: insights using high-resolution coherent mapping
research-article
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
A 75-year-old woman with hypertrophic cardiomyopathy and symptomatic atrial tachycardia
(AT) was admitted for first-time catheter ablation (Supplementary material online,
Figure S1
). Entrainment during AT-1 (cycle length: CL = 230 ms) from both the left atrial (LA)
roof and mitral annulus (MA) revealed that both sites were within the circuit. A high-resolution
electroanatomic map of the left atrium was created using a PentaRay catheter with
the CARTO mapping system (Biosense Webster, Diamond Bar, CA, USA). Activation mapping
was performed, and the Coherent module (CARTO, Biosense Webster, Diamond Bar, CA,
USA) was used to display the colour and conduction velocity vectors for the electrical
wave propagation.
1
Video 1 shows the Coherent propagation map during AT-1, which was consistent with
a dual loop macroreentry with roof-dependent and MA circuits. After creation of a
linear ablation lesion set from the MA to the anterior left superior pulmonary vein,
AT-1 transformed to another AT (AT-2, Supplementary material online,
Figure S2
) with a different propagation pattern. Activation mapping of the endocardial LA clearly
demonstrated that the activation started from the summit of a large diverticulum on
the LA roof (
Figure 1
,
2
, Supplementary material online,
Figure S3
), propagating to its base and then the left atrium and right atrium (Video 2). The
mapped propagation time in the left atrium was 235 ms, which did not cover the total
AT-2 CL (265 ms), and the 30 ms difference was regarded as the conduction time through
the epicardial tissue. Entrainment mapping demonstrated that the circuit of AT-2 included
the proximal and distal coronary sinus and diverticulum (Supplementary material online,
Figures S4 and S5). Therefore, like AT-1, AT-2 was speculated to also be a counter
clockwise perimitral atrial flutter. Since the endocardial aspect of the left atrium
was blocked, propagation was felt to use epicardial connections along the anterior
LA wall utilizing the diverticulum before entering the endocardial left atrium. AT-2
was terminated during radiofrequency catheter ablation around the base of diverticulum,
after which AT-2 was rendered non-inducible. Voltage mapping demonstrated large areas
of bipolar voltage abnormality at the anterior and perimitral LA (Supplementary material
online,
Figure S6
), and which may have provided the substrate for sustaining tachycardia. High-density
Coherent mapping was able to visualize the circuit of an unusual macroreentrant AT
utilizing an epicardial connection associated with an LA roof diverticulum, which
to the best of our knowledge, has not been previously reported.
Figure 1
Computed tomography of the LA and a large diverticulum (anterior–posterior view).
LA, left atrium; LAA, left atrial appendage; LSPV, left superior pulmonary vein; RIPV,
right inferior pulmonary vein; RSPV, right superior pulmonary vein.
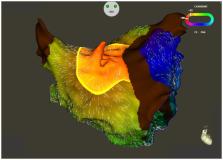
Figure 2
Coherent propagation map during AT-2.
Supplementary material
Supplementary material is available at European Heart Journal - Case Reports online.
Supplementary Material
ytaa268_Supplementary_Data
Click here for additional data file.
Related collections
Most cited references1

- Record: found
- Abstract: found
- Article: found
Identification of critical isthmus using coherent mapping in patients with scar‐related atrial tachycardia
Jennifer Vicera, Yenn-Jiang Lin, Po-Tseng Lee … (2020)