- Record: found
- Abstract: found
- Article: found
A comparison between ketorolac and nefopam as adjuvant analgesics for postoperative patient-controlled analgesia: a randomized, double-blind, prospective study
Read this article at
Abstract
Background
We compared the analgesic efficacy and side effects of ketorolac and nefopam that were co-administered with fentanyl via intravenous patient-controlled analgesia.
Methods
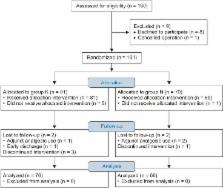
One hundred and sixty patients scheduled for laparoscopic cholecystectomy were randomly assigned to ketorolac (Group K) or nefopam (Group N) groups. The anesthetic regimen was standardized for all patients. The analgesic solution contained fentanyl 600 µg and ketorolac 180 mg in Group K, and fentanyl 600 µg and nefopam 120 mg in Group N. The total volume of analgesic solution was 120 ml. Postoperative analgesic consumption, recovery of pulmonary function, and pain intensities at rest and during the forced expiration were evaluated at postoperative 2, 6, 24, and 48 h. The postoperative side effects of analgesics were recorded.
Results
Cumulative postoperative analgesic consumptions at postoperative 48 h were comparable (Group K: 93.4 ± 24.0 ml vs. Group N: 92.9 ± 26.1 ml, P = 0.906) between the groups. Pain scores at rest and during deep breathing were similar at the time of each examination. The recovery of pulmonary function showed no significant differences between the groups. Overall, postoperative nausea and vomiting incidence was higher in Group N compared with Group K (59% vs. 34%, P = 0.015). The other side effects were comparable between both groups.
Conclusions
Analgesic efficacies of ketorolac and nefopam that were co-administered with fentanyl for postoperative pain management as adjuvant analgesics were similar. However, postoperative nausea and vomiting incidence was higher in the nefopam-fentanyl combination compared with the ketorolac-fentanyl combination.
Related collections
Most cited references29
- Record: found
- Abstract: found
- Article: not found
A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers.
- Record: found
- Abstract: found
- Article: not found
Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs for the reduction in morphine-related side-effects after major surgery: a systematic review.
- Record: found
- Abstract: found
- Article: not found