- Record: found
- Abstract: found
- Article: found
Influence of predicting the diagnosis from history on the accuracy of physical examination
Read this article at
Abstract
Background
This study aimed to clarify the influence of predicting a correct diagnosis from the history on physical examination by comparing the diagnostic accuracy of auscultation with and without clinical information.
Methods
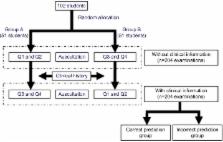
The participants were 102 medical students from the 2013 clinical clerkship course. Auscultation was performed with a cardiology patient simulator. Participants were randomly assigned to two groups. Each group listened to a different simulated heart murmur and then made a diagnosis without clinical information. Next, a history suggesting a different murmur was provided to each group and they predicted the diagnosis. Finally, the students listened to a murmur corresponding to the history provided and again made a diagnosis. Correct and incorrect diagnosis rates of auscultation were compared between students with and without clinical information, between students predicting a correct or incorrect diagnosis from the history (correct and incorrect prediction groups, respectively), and between students without clinical information and those making an incorrect prediction.
Results
For auscultation with or without clinical information, the correct diagnosis rate was 62.7% (128/204 participants) versus 54.4% (111/204 participants), showing no significant difference ( P=0.09). After receiving clinical information, a correct diagnosis was made by 102/117 students (87.2%) in the correct prediction group versus 26/87 students (29.9%) in the incorrect prediction group, showing a significant difference ( P=0.006). The correct diagnosis rate was also significantly lower in the incorrect prediction group than when the students performed auscultation without clinical information (54.4% versus 29.9%, P<0.001).
Conclusion
Obtaining a history alone does not improve the diagnostic accuracy of physical examination. However, accurately predicting the diagnosis from the history is associated with higher diagnostic accuracy of physical examination, while incorrect prediction is associated with lower diagnostic accuracy of examination.
Related collections
Most cited references16
- Record: found
- Abstract: found
- Article: not found
Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims.
- Record: found
- Abstract: found
- Article: not found
Dual processing and diagnostic errors.
- Record: found
- Abstract: found
- Article: not found