- Record: found
- Abstract: found
- Article: found
Determination of Antimicrobial Prescribing Practices in an Integrated Health System Emergency Department
Read this article at
Abstract
Introduction
Antibiotic stewardship utilizes interprofessional collaborative practices, including professionals from medicine, pharmacy, nursing, social services, and clinical laboratory science, to identify potential problems proactively. A tertiary care integrated health system’s Emergency Department (ED) aimed to identify antimicrobials prescribed to the outpatient community as part of a proactive antimicrobial stewardship project.
Methods
A pilot, prospective, snapshot of a tertiary community hospital’s outpatient antimicrobial prescribing habits was conducted. All subjects were identified via a daily report of patients discharged from the ED over 30 days in the summer of 2017 and individually reviewed for prescribed antimicrobial(s). Exclusions were hospital admission, antimicrobial sensitivity, and antimicrobial courses less than five days or more than 14 days. The primary goal was determining the number of antimicrobial oral tablets/capsule prescriptions to adult outpatients within a 5 to 14-day treatment window. Secondary goals were to include the diagnosis, non-capsule/tablet antimicrobial, pediatric patients, and prescriptions outside the treatment window.
Results
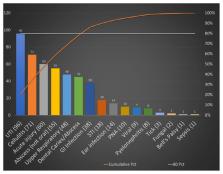
Total number of antimicrobial prescriptions over the 30-day period was 653 in 5,520 individual visits. Total number of adults prescribed oral antimicrobials was 467 (15.6 daily). Patients were diagnosed with infections including urinary tract, cellulitis, soft tissue injury, abscess, upper respiratory, dental caries, gastrointestinal, sexually transmitted, otitis media/externa, pneumonia, viral, pyelonephritis, tick-borne, fungal, Bell’s Palsy, and sepsis. The number of non-adult, non-oral, and outside window treatment antimicrobial prescriptions were 186 (6.2 daily). With an average 184 patients treated in the ED daily, approximately 11.8% received antimicrobial treatment on discharge.
Conclusion
Important aspects of the project were the evaluation of antimicrobial prescribing habits for a midwest ED and identification of potential complications requiring future interventions for follow-up or preventative measures to assist in patient care and community health. Areas of practice improvement were identified inadvertently as a result of this project. Potential future studies included seasonal variability, whether the patient obtained a prescription and complied with treatment, and differences between inpatient and outpatient antimicrobial prescribing practices.
Related collections
Most cited references3
- Record: found
- Abstract: found
- Article: not found
Communication gaps and readmissions to hospital for patients aged 75 years and older: observational study.
- Record: found
- Abstract: found
- Article: not found
Assessments of Opportunities to Improve Antibiotic Prescribing in an Emergency Department: A Period Prevalence Survey
- Record: found
- Abstract: found
- Article: not found