- Record: found
- Abstract: found
- Article: found
Extracorporeal support for pulmonary resection: current indications and results
Read this article at
Abstract
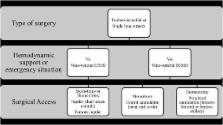
Extracorporeal assistances are exponentially used for patients, with acute severe but reversible heart or lung failure, to provide more prolonged support to bridge patients to heart and/or lung transplantation. However, experience of use of extracorporeal assistance for pulmonary resection is limited outside lung transplantation. Airways management with standard mechanical ventilation system may be challenging particularly in case of anatomical reasons (single lung), presence of respiratory failure (ARDS), or complex tracheo-bronchial resection and reconstruction. Based on the growing experience during lung transplantation, more and more surgeons are now using such devices to achieve good oxygenation and hemodynamic support during such challenging cases. We review the different extracorporeal device and attempt to clarify the current practice and indications of extracorporeal support during pulmonary resection.
Related collections
Most cited references46
- Record: found
- Abstract: not found
- Article: not found
Multidisciplinary management of lung cancer.
- Record: found
- Abstract: found
- Article: not found
Extracorporeal membrane oxygenation in cardiopulmonary disease in adults.
- Record: found
- Abstract: found
- Article: not found