- Record: found
- Abstract: found
- Article: found
Outcomes in Asymptomatic Severe Aortic Stenosis With Preserved Ejection Fraction Undergoing Rest and Treadmill Stress Echocardiography
Read this article at
Abstract
Background
In asymptomatic patients with severe aortic stenosis and preserved left ventricular ejection fraction, we sought to assess the incremental prognostic value of resting valvuloarterial impedence (Zva) and left ventricular global longitudinal strain ( LV‐ GLS) to treadmill stress echocardiography.
Methods and Results
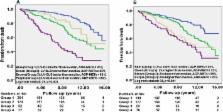
We studied 504 such patients (66±12 years, 78% men, 32% with coronary artery disease who underwent treadmill stress echocardiography between 2001 and 2012. Clinical and exercise variables (% of age‐sex predicted metabolic equivalents [% AGP‐ METs]) were recorded. Resting Zva ([systolic arterial pressure+mean aortic valve gradient]/[ LV‐stroke volume index]) and LV‐ GLS (measured offline using Velocity Vector Imaging, Siemens) were obtained from the baseline resting echocardiogram. Death was the primary outcome. There were no major adverse cardiac events during treadmill stress echocardiography. Indexed aortic valve area, Zva, and LV‐ GLS were 0.46±0.1 cm 2/m 2, 4.5±0.9 mm Hg/mL per m 2 and −16±4%, respectively; only 50% achieved >100% AGP‐ METs. Sixty‐four percent underwent aortic valve replacement. Death occurred in 164 (33%) patients over 8.9±3.6 years (2 within 30 days of aortic valve replacement). On multivariable Cox survival analysis, higher Society of Thoracic Surgeons score (hazard ratio or HR 1.06), lower % AGP‐ METS ( HR 1.16), higher Zva ( HR 1.25) and lower LV‐ GLS ( HR 1.12) were associated with higher longer‐term mortality, while aortic valve replacement ( HR 0.45) was associated with improved survival (all P<0.01). Sequential addition of ZVa and LV‐ GLS to clinical model (Society of Thoracic Surgeons score and % AGP‐ METs) increased the c‐statistic from 0.65 to 0.69 and 0.75, respectively, both P<0.001); findings were similar in the subgroup of patients who underwent aortic valve replacement.
Related collections
Most cited references27
- Record: found
- Abstract: not found
- Article: not found
American Society of Echocardiography recommendations for performance, interpretation, and application of stress echocardiography.
- Record: found
- Abstract: found
- Article: not found
Impaired chronotropic response to exercise stress testing as a predictor of mortality.
- Record: found
- Abstract: found
- Article: not found