- Record: found
- Abstract: found
- Article: found
Morphea induced by SARS‐CoV‐2 infection: A case report
letter
Flavia Pigliacelli , MD
1 ,
Alessia Pacifico , MD
1 ,
Maria Mariano , MD
1
,
,
Andrea D’Arino , MD
1 ,
Antonio Cristaudo , MD
1 ,
Paolo Iacovelli , MD
1
15 November 2021
Read this article at

There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Dear Editor,
The widespread diffusion of severe acute respiratory syndrome coronavirus‐2 (SARS‐CoV‐2),
a member of the coronavirus family responsible for Coronavirus disease (COVID‐19),
is still in the headlines for the impressive health and economic burden worldwide.
The immune response against this novel virus is still undergoing extensive research,
and the possible long‐term outcomes remain basically unknown. Immunity plays a key
role in the defense against several microorganisms, and SARS‐CoV‐2 is no different.
The infections can result in a hyperactive immune response with excessive inflammatory
reactions.
1
These are generally accompanied by the release of impressive amounts of proinflammatory
cytokines, an event known as “cytokine storm,” that is correlated with lung damage,
organ failure, and a negative prognosis.
2
,
3
The possibility that these immunologic derangements could result in the induction
and/or the exacerbation of other immune‐mediated diseases, including cutaneous ones,
has not been completely investigated.
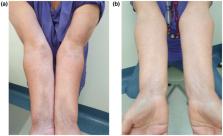
We report the case of a 61‐year‐old female patient referred to our dermatologic department
for the development of asymptomatic bilateral sclerotic cutaneous lesions on the forearms
which appeared 2 months before. The physical examination revealed the presence of
several brownish and violaceous plaques with mild erythematous borders on forearms,
with sclerotic appearance, partially tending to confluence. The lesions showed a symmetrical
and bilateral distribution and were about 5–10 cm in diameter (Fig. 1a). The patient
referred that the skin manifestations started about 1 month after the dismissal from
hospitalization for COVID‐19 pneumonia (confirmed through RT‐PCR). Her familiar and
personal history was negative for autoimmune and chronic inflammatory skin disorders.
On suspicion of localized morphea, blood examination tests and skin biopsy were performed.
Blood tests, including antinuclear antibodies (ANA), antibodies to single‐stranded
DNA (a‐ssDNA), autoantibodies to extractable nuclear antigens (ENAs), and COVID‐19
swab test, were negative excluding systemic involvement. Histological examination
revealed the presence of thin epidermis with moderate dermal sclerosis and thickening
of collagen fibers, confirming the diagnosis of morphea.
Figure 1
Clinical manifestations: (a) the presence of several brownish and violaceous plaques
with mild erythematous borders on forearms, with sclerotic appearance, partially tending
to confluence. (b) Complete clinical resolution after 16 weeks of treatment with clobetasol
ointment and vitamin E emollient
A topical therapy with a high‐potency steroid (clobetasol ointment) and vitamin E
emollient was started, with a remarkable improvement after 8 weeks and a complete
clinical resolution after 16 weeks of treatment (Fig. 1b).
Morphea, also known as localized scleroderma, is an inflammatory skin condition that
is characterized by the presentation of single or multiple inflammatory or sclerotic
plaques.
4
While the pathogenesis remains largely unknown, several factors can contribute to
the emergence of autoimmune disease including the genetic predisposition, environmental
triggers such as bacterial and viral infections, and intrinsic factors, such as hormonal
and immunologic dysregulation.
5
In this case, the negative personal anamnesis for autoimmune disorders and the development
of cutaneous manifestations after COVID‐19 infection suggested a possible link between
autoimmune disease and SARS‐CoV‐2. Some authors proposed that SARS‐CoV‐2 could act
as a trigger in the development of organ‐specific autoimmune disorders, in genetic
predisposed subjects.
6
In particular, a molecular mimicry phenomenon between virus and human protein has
been hypothesized. Hence, the exaggerated activation of immune system against the
virus could induce a cross‐reaction with auto‐antigens in common with viral peptides,
leading to an autoimmune dysfunction.
7
Recently, some authors reported the development and/or worsening of inflammatory skin
diseases after COVID‐19 infection, such as atopic dermatitis
8
and psoriasis,
9
induced by abnormal activation of the immune system in response to virus and consequent
inflammatory pathways.
To the best of our knowledge, in the literature, there are no reports of morphea triggered
by COVID‐19 infection. We report this case to underline the importance of this clinical
condition during the COVID‐19 pandemic for the dermatologists, in order to provide
a proper diagnosis and a correct therapeutic management.
Related collections
Most cited references10
- Record: found
- Abstract: found
- Article: not found
Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China
Chaolin Huang, Yeming Wang, Xingwang Li … (2020)
- Record: found
- Abstract: found
- Article: not found
Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China
Qiurong Ruan, Kun Yang, Wenxia Wang … (2020)
- Record: found
- Abstract: found
- Article: found
The COVID-19 Cytokine Storm; What We Know So Far
Dina Ragab, Haitham Salah Eldin, Mohamed Taeimah … (2020)