- Record: found
- Abstract: found
- Article: found
Epstein-Barr virus-associated post-transplant lymphoproliferative disorders: beyond chemotherapy treatment
Read this article at
Abstract
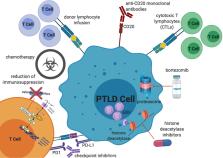
Post-transplant lymphoproliferative disorder (PTLD) is a rare but life-threatening complication of both allogeneic solid organ (SOT) and hematopoietic cell transplantation (HCT). The histology of PTLD ranges from benign polyclonal lymphoproliferation to a lesion indistinguishable from classic monoclonal lymphoma. Most commonly, PTLDs are Epstein-Barr virus (EBV) positive and result from loss of immune surveillance over EBV. Treatment for PTLD differs from the treatment for typical non-Hodgkin lymphoma because prognostic factors are different, resistance to treatment is unique, and there are specific concerns for organ toxicity. While recipients of HCT have a limited time during which they are at risk for this complication, recipients of SOT have a lifelong requirement for immunosuppression, so approaches that limit compromising or help restore immune surveillance are of high interest. Furthermore, while EBV-positive and EBV-negative PTLDs are not intrinsically resistant to chemotherapy, the poor tolerance of chemotherapy in the post-transplant setting makes it essential to minimize potential treatment-related toxicities and explore alternative treatment algorithms. Therefore, reduced-toxicity approaches such as single-agent CD20 monoclonal antibodies or bortezomib, reduced dosing of standard chemotherapeutic agents, and non-chemotherapy-based approaches such as cytotoxic T cells have all been explored. Here, we review the chemotherapy and non-chemotherapy treatment landscape for PTLD.
Related collections
Most cited references129
- Record: found
- Abstract: found
- Article: not found
PD-1 Blockade in Tumors with Mismatch-Repair Deficiency.
- Record: found
- Abstract: found
- Article: not found
Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification.
- Record: found
- Abstract: found
- Article: not found