- Record: found
- Abstract: found
- Article: not found
The CNCDs and the NTDs: Blurring the Lines Dividing Noncommunicable and Communicable Chronic Diseases
editorial
29 October 2008
Read this article at

There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
World Health Organization statistics show that deaths worldwide from chronic noncommunicable
diseases (CNCDs) now exceed those from infectious diseases [1]. The major CNCDs causing
the greatest share of deaths and disability worldwide include cardiovascular conditions
(mainly heart disease and stroke), some cancers, chronic respiratory conditions, and
type 2 diabetes [2]. Together they account for 60% of all deaths worldwide [2]. Approximately
80% of the CNCD deaths occur in low-income and middle-income countries [2]. Most of
the factors contributing to such large numbers of deaths, a large proportion of which
are premature, are similar to those in developed countries. They include increasing
tobacco use, diminished physical activity and lack of exercise, and the consumption
of unhealthy foods [2].
CNCDs are defined as diseases or conditions that affect individuals over an extensive
period of time and for which there are no known causative agents that are transmitted
from one affected individual to another [2]. More than any other type of infection,
the neglected tropical diseases (NTDs) most closely resemble the CNCDs. The characteristic
feature of the NTDs are their chronic and insidious clinical manifestations, and the
resulting long-term disability [3],[4]. An impoverished person suffering from a NTD
will typically have the condition for years, sometimes decades, and sometimes their
entire life [3],[4]. Indeed, except for the fact that we know their causative agents,
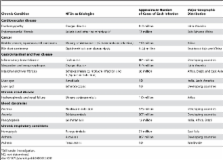
the NTDs for the most part meet CNCD-defining criteria. Shown in Table 1 are the major
chronic disease syndromes that result from NTDs. Chagas disease is a leading cause
of chronic cardiovascular disease in Latin America, often resulting in severe cardiomyopathy
[5], while Loa loa and other parasitic infections have been identified as possible
etiologies of endomyocardial fibrosis in sub-Saharan Africa [6]. Urinary schistosomiasis
is a leading cause of bladder cancer in Africa and the Middle East (causing a unique
squamous cell carcinoma) [7],[8], while opisthorchiasis and clonorchiasis, both causes
of oriental liver fluke infection, cause bile duct carcinoma in Southeast Asia and
China [9]. Worldwide, trichuriasis causes more inflammatory bowel disease than either
Crohn disease or ulcerative colitis [10], and schistosomiasis is a leading cause of
chronic renal disease and failure in Africa and the Middle East [7],[8],[11]. In Asia,
paragonomiasis ranks with tuberculosis and lung cancer as a leading cause of hemoptysis
[12], and toxocariasis is emerging as an important cause of asthma [13].
10.1371/journal.pntd.0000312.t001
Table 1
CNCD-Like Syndromes Caused by the NTDs.
Chronic Condition
NTDs as Etiologies
Approximate Number of Cases of Each Infection
Major Geographic Distribution
Cardiovascular disease
Cardiomyopathy
Chagas disease
8–9 million
Latin America
Endomyocardial fibrosis
Loiasis (and other helminthiases)a
13 million
Sub-Saharan Africa
Cancer
Bladder cancer; squamous cell carcinoma
Urinary schistosomiasis (S. haematobium infection)
119 million
Africa
Bile duct carcinoma
Opisthorchiasis and clonorchiasis
6–44 million
Southeast Asia and China
Gastrointestinal and liver disease
Inflammatory bowel disease
Trichuriasis
604 million
Developing countries
Megacolon and megaesophagus
Chagas disease
8–9 million
Latin America
Intestinal and liver fibrosis
Schistosomiasis (S. mansoni infection and S. japonicum infection)
68 million
Africa, Brazil, and East Asia
Liver cyst
Amebiasis
ND
India, Latin America
Liver cyst
Echinococcosis
ND
Developing countries
Chronic renal disease
Hydronephrosis and renal failure
Urinary schistosomiasis
119 million
Africa
Blood dyscrasias
Anemia
Hookworm infection
576 million
Developing countries
Anemia
Schistosomiasis
207 million
Developing countries
Pancytopenia
Leishmaniasis
12 million
India, Africa, Brazil
Chronic respiratory conditions
Hemoptysis
Paragonimiasis
21 million
East Asia
Asthma
Ascariasis
807 million
Developing countries
Asthma
Toxocariasis
ND
Worldwide
a
Still under investigation.
ND, not determined.
Anemia is one of the best documented examples of a chronic condition in which a single
NTD, such as hookworm infection, accounts for a significant percentage of the attributable
risk [14]–[17], or in which multiple NTD coinfections and polyparasitism make a significant
contribution [18]–[23]. Another is cancer—urinary schistosomiasis was shown to account
for 28% of the bladder cancer in Bulawayo, Zimbabwe [24], and 0.1% of the world's
cancer burden [25], while liver flukes (e.g., Clonorchis sinensis and Opisthorchis
spp.) account for an estimated 0.02% of all cancers [25]. Van der Werf et al. determined
that Schistosoma haematobium was responsible for 10 million cases of hydronephrosis
in sub-Saharan Africa, and S. mansoni was associated with 8.5 million cases of hepatomegaly
in the region [11]. It has been further estimated that approximately 5.4 million people
will develop chronic Chagas heart disease, while 900,000 will develop severe enlargement
of the digestive tract (megacolon and megaesophagus) [26].
However, the full extent to which the NTDs listed in Table 1 contribute to the other
CNCDs requires active investigation. Among the bottom billion living in the poorest
areas of the developing world, the underlying causes of chronic cardiovascular, renal,
hepatic, and gastrointestinal disease, as well as cancer, are frequently neglected
and unstudied. Because they are so common in low-income and middle-income countries,
it is of critical importance to determine how the NTDs contribute significantly to
the CNCD burden in such regions. Such an evidence base is critical for informing new
policies for tackling chronic disease in developing countries. The new Grand Challenges
in CNCDs initiative [2] is an ambitious effort to raise public awareness of these
conditions in the developing world, enhance economic, legal, and environmental policies,
modify risk factors, mitigate the health impacts of poverty and urbanization, engage
the community, and reorient health systems away from treatment towards prevention
[2]. Wherever the NTDs geographically overlap with the CNCDs, there is a need to assess
the contribution of the former, and to recognize that when it comes to NTDs, the distinction
between noncommunicable and communicable diseases can be murky.
Related collections
Most cited references19
- Record: found
- Abstract: not found
- Article: not found
Control of neglected tropical diseases.
Peter Hotez, David H. Molyneux, Alan Fenwick … (2007)
- Record: found
- Abstract: found
- Article: not found
Incorporating a Rapid-Impact Package for Neglected Tropical Diseases with Programs for HIV/AIDS, Tuberculosis, and Malaria
Peter Hotez, David H. Molyneux, Alan Fenwick … (2006)
- Record: found
- Abstract: found
- Article: not found
Pathogenesis of chronic Chagas heart disease.
José Marin-Neto, Edecio Cunha-Neto, Benedito Maciel … (2007)