- Record: found
- Abstract: found
- Article: not found
Monitoring SARS-CoV-2 in air and on surfaces and estimating infection risk in buildings and buses on a university campus
Read this article at

Abstract
Background
Evidence is needed on the presence of SARS-CoV-2 in various types of environmental samples and on the estimated transmission risks in non-healthcare settings on campus.
Objectives
The objective of this research was to collect data on SARS-CoV-2 viral load and to examine potential infection risks of people exposed to the virus in publicly accessible non-healthcare environments on a university campus.
Methods
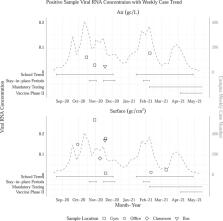
Air and surface samples were collected using wetted wall cyclone bioaerosol samplers and swab kits, respectively, in a longitudinal environmental surveillance program from August 2020 until April 2021 on the University of Michigan Ann Arbor campus. Quantitative rRT-PCR with primers and probes targeting gene N1 were used for SARS-CoV-2 RNA quantification. The RNA concentrations were used to estimate the probability of infection by quantitative microbial risk assessment modeling and Monte-Carlo simulation.
Results
In total, 256 air samples and 517 surface samples were collected during the study period, among which positive rates were 1.6% and 1.4%, respectively. Point-biserial correlation showed that the total case number on campus was significantly higher in weeks with positive environmental samples than in non-positive weeks ( p = 0.001). The estimated probability of infection was about 1 per 100 exposures to SARS-CoV-2-laden aerosols through inhalation and as high as 1 per 100,000 exposures from contacting contaminated surfaces in simulated scenarios.
Significance
Viral shedding was demonstrated by the detection of viral RNA in multiple air and surface samples on a university campus. The low overall positivity rate indicated that the risk of exposure to SARS-CoV-2 at monitored locations was low. Risk modeling results suggest that inhalation is the predominant route of exposure compared to surface contact, which emphasizes the importance of protecting individuals from airborne transmission of SARS-CoV-2 and potentially other respiratory infectious diseases.
Impact
Given the reoccurring epidemics caused by highly infectious respiratory viruses in recent years, our manuscript reinforces the importance of monitoring environmental transmission by the simultaneous sampling and integration of multiple environmental surveillance matrices for modeling and risk assessment.
Related collections
Most cited references38
- Record: found
- Abstract: found
- Article: not found
Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study
- Record: found
- Abstract: found
- Article: not found
Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1
- Record: found
- Abstract: found
- Article: not found