- Record: found
- Abstract: found
- Article: found
Prevalence, Risk Factors, and Pathophysiology of Dysglycemia among People Living with HIV in Sub-Saharan Africa
Read this article at
Abstract
Objective
To review available literature on the prevalence, risk factors, pathophysiology, and clinical outcomes of dysglycemia among people living with HIV (PLHIV) in sub-Saharan Africa (SSA).
Methods
Database search on PUBMED for eligible studies describing the prevalence, risk factors, pathophysiology, or clinical outcomes of dysglycemia in SSA PLHIV.
Results
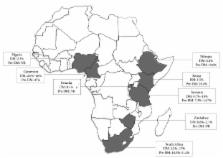
Prevalence of diabetes mellitus (DM) and pre-DM among SSA PLHIV ranged from 1% to 26% and 19% to 47%, respectively, in 15 identified studies. Older age and an elevated body mass index (BMI) were common risk factors for dysglycemia. Risk factors potentially more specific to PLHIV in SSA included exposure to older-generation thymidine analogues or protease inhibitors, malnutrition at ART initiation, a failure to gain fat mass on treatment, and elevated serum lipids. There is evidence of higher nephropathy and neuropathy rates among PLHIV in SSA with comorbid DM compared to HIV-negative individuals with DM.
Conclusion
There is a need for longitudinal studies to enhance understanding of the risk factors for dysglycemia among PLHIV in SSA, further research into optimal therapies to reduce pre-DM progression to DM among SSA PLHIV, and studies of the burden and phenotype of diabetic complications and other health outcomes among PLHIV with comorbid DM in SSA.
Related collections
Most cited references76
- Record: found
- Abstract: found
- Article: not found
Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013.
- Record: found
- Abstract: found
- Article: not found