- Record: found
- Abstract: found
- Article: found
The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials
Read this article at
Abstract
Introduction
Dynamic predictors of fluid responsiveness, namely systolic pressure variation, pulse pressure variation, stroke volume variation and pleth variability index have been shown to be useful to identify in advance patients who will respond to a fluid load by a significant increase in stroke volume and cardiac output. As a result, they are increasingly used to guide fluid therapy. Several randomized controlled trials have tested the ability of goal-directed fluid therapy (GDFT) based on dynamic parameters (GDFTdyn) to improve post-surgical outcome. These studies have yielded conflicting results. Therefore, we performed this meta-analysis to investigate whether the use of GDFTdyn is associated with a decrease in post-surgical morbidity.
Methods
A systematic literature review, using MEDLINE, EMBASE, and The Cochrane Library databases through September 2013 was conducted. Data synthesis was obtained by using odds ratio (OR) and weighted mean difference (WMD) with 95% confidence interval (CI) by random-effects model.
Results
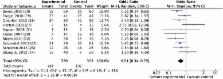
In total, 14 studies met the inclusion criteria (961 participants). Post-operative morbidity was reduced by GDFTdyn (OR 0.51; CI 0.34 to 0.75; P <0.001). This effect was related to a significant reduction in infectious (OR 0.45; CI 0.27 to 0.74; P = 0.002), cardiovascular (OR 0.55; CI 0.36 to 0.82; P = 0.004) and abdominal (OR 0.56; CI 0.37 to 0.86; P = 0.008) complications. It was associated with a significant decrease in ICU length of stay (WMD −0.75 days; CI −1.37 to −0.12; P = 0.02).
Related collections
Most cited references39
- Record: found
- Abstract: not found
- Article: not found
The hazards of scoring the quality of clinical trials for meta-analysis.
- Record: found
- Abstract: found
- Article: not found
Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure.
- Record: found
- Abstract: found
- Article: not found