- Record: found
- Abstract: found
- Article: found
Impact of diet on ten-year absolute cardiovascular risk in a prospective cohort of 94 321 individuals: A tool for implementation of healthy diets

Read this article at
Summary
Background
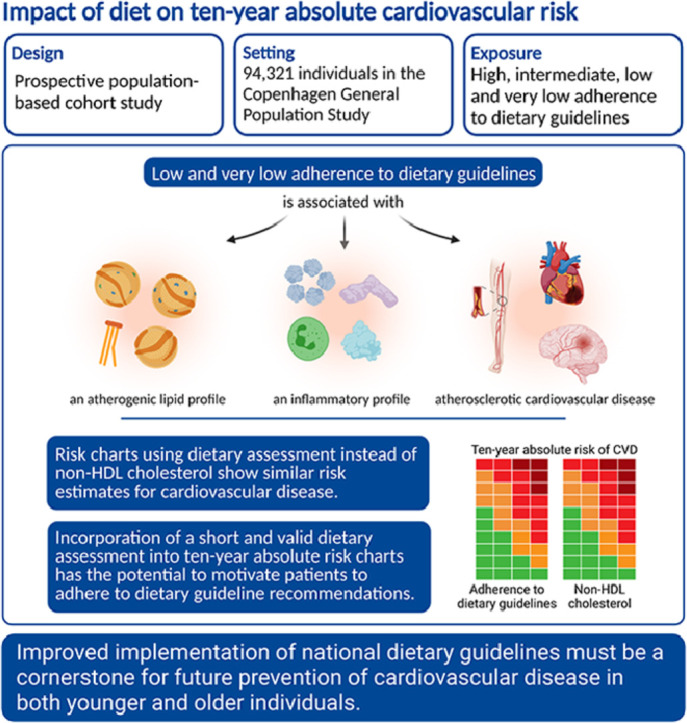
An unhealthy diet is a major risk factor for cardiovascular disease attributing to the burden of non-communicable diseases. Current dietary guidelines are not sufficiently implemented and effective strategies to encourage people to change and maintain healthy diets are lacking. We aimed to evaluate the impact of incorporating dietary assessment into ten-year absolute risk charts for atherosclerotic cardiovascular disease (ASCVD).
Methods
In the prospective Copenhagen General Population Study including 94 321 individuals, we generated sex-specific ten-year absolute risk scores for ASCVD according to adherence to dietary guidelines, using a short and valid food frequency questionnaire. To account for competing risk, we used the method of Fine-Gray.
Findings
Non-adherence to dietary guidelines was associated with an atherogenic lipid and inflammatory profile. Ten-year absolute risk of ASCVD increased with increasing age, increasing systolic blood pressure, and decreasing adherence to dietary guidelines for both sexes. The highest ten-year absolute risk of ASCVD of 38% was observed in men aged 65–69 years who smoked, had very low adherence to dietary guidelines, and a systolic blood pressure between 160 and 179 mmHg. The corresponding value for women was 26%. Risk charts replacing dietary assessment with non-HDL cholesterol yielded similar estimates.
Interpretation
Incorporation of a short dietary assessment into ten-year absolute risk charts has the potential to motivate patients to adhere to dietary guideline recommendations. Improved implementation of national dietary guidelines must be a cornerstone for future prevention of cardiovascular disease in both younger and older individuals.
Graphical abstract
Related collections
Most cited references35

- Record: found
- Abstract: found
- Article: found
Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019

- Record: found
- Abstract: found
- Article: found
Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019

- Record: found
- Abstract: found
- Article: found