- Record: found
- Abstract: found
- Article: found
P-wave indices in patients with pulmonary emphysema: do P-terminal force and interatrial block have confounding effects?
Abstract
Introduction
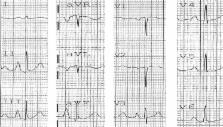
Pulmonary emphysema causes several electrocardiogram changes, and one of the most common and well known is on the frontal P-wave axis. P-axis verticalization (P-axis > 60°) serves as a quasidiagnostic indicator of emphysema. The correlation of P-axis verticalization with the radiological severity of emphysema and severity of chronic obstructive lung function have been previously investigated and well described in the literature. However, the correlation of P-axis verticalization in emphysema with other P-indices like P-terminal force in V 1 (Ptf), amplitude of initial positive component of P-waves in V 1 (i-PV1), and interatrial block (IAB) have not been well studied. Our current study was undertaken to investigate the effects of emphysema on these P-wave indices in correlation with the verticalization of the P-vector.
Materials and methods
Unselected, routinely recorded electrocardiograms of 170 hospitalized emphysema patients were studied. Significant Ptf (s-Ptf) was considered ≥40 mm.ms and was divided into two types based on the morphology of P-waves in V 1: either a totally negative (−) P wave in V 1 or a biphasic (+/−) P wave in V 1.
Results
s-Ptf correlated better with vertical P-vectors than nonvertical P-vectors ( P = 0.03). s-Ptf also significantly correlated with IAB ( P = 0.001); however, IAB and P-vector verticalization did not appear to have any significant correlation ( P = 0.23). There was a very weak correlation between i-PV1 and frontal P-vector ( r = 0.15; P = 0.047); however, no significant correlation was found between i-PV1 and P-amplitude in lead III ( r = 0.07; P = 0.36).
Conclusion
We conclude that increased P-tf in emphysema may be due to downward right atrial position caused by right atrial displacement, and thus the common assumption that increased P-tf implies left atrial enlargement should be made with caution in patients with emphysema. Also, the lack of strong correlation between i-PV1 and P-amplitude in lead III or vertical P-vector may suggest the predominant role of downward right atrial distortion rather than right atrial enlargement in causing vertical P-vector in emphysema.
Most cited references19
- Record: found
- Abstract: found
- Article: not found
Interatrial blocks. A separate entity from left atrial enlargement: a consensus report.
- Record: found
- Abstract: found
- Article: not found
Electromechanical dysfunction of the left atrium associated with interatrial block.
- Record: found
- Abstract: not found
- Article: not found