- Record: found
- Abstract: found
- Article: found
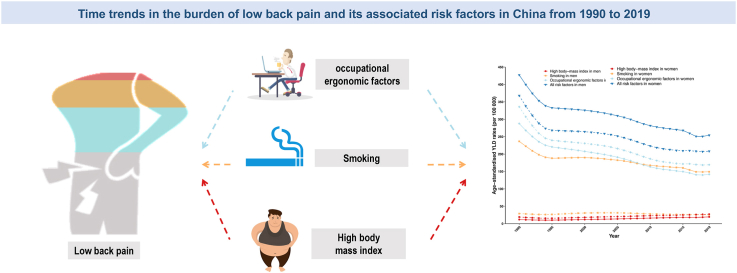
Time trends in the burden of low back pain and its associated risk factors in China from 1990 to 2019

Read this article at
Abstract
Background
From 1990 to 2019, low back pain (LBP) was the leading cause of years lived with disability (YLDs) in China. However, the change patterns of LBP and its risk factors in China remain unclear.
Methods
Data from the Global Burden of Disease Study 2019 were used. We used the join-point regression model and age-period-cohort analysis to evaluate the time trends of attributable risk factors on the burden of LBP.
Results
In 2019, the risk factors included in this analysis accounted for 4.36 million YLDs of LBP, representing 42.2% of all YLDs of LBP in China, with 2.86 million due to occupational ergonomic factors, 1.74 million due to smoking, and 0.46 million due to high body mass index (BMI). The age-standardized YLD rates of LBP showed downward trends during 1990–2019, while there was a faster decline between 1990 and 1994. The curves of local drifts, which reflected the average annual percentage change across age groups, showed an increasing trend with age for high BMI and smoking, and a downward trend for occupational ergonomic factors. The YLD rates for LBP increased dramatically with age for high BMI, while it reached a peak at 40–60 years old for occupational ergonomic factors, and 65–80 years old for smoking. The period and cohort rate ratios of LBP YLD decreased in the past 3 decades for occupational ergonomic factors and smoking, while increased for high BMI.
Conclusions
Our results provided strong evidence that there were diverse changing patterns for different risk factors, highlighting the need for risk-specific strategies.
The translational potential of this article
China has the largest senior population and the fastest aging population in the world. Given that LBP typically occurs in the senior population, there would be an increasing LBP burden on China's health system. This suggests that effective strategies for LBP prevention should be strictly implemented in China, particularly in the senior population, which is of crucial translational potential.
Graphical abstract
Related collections
Most cited references24

- Record: found
- Abstract: found
- Article: found
Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019

- Record: found
- Abstract: found
- Article: found
Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019

- Record: found
- Abstract: found
- Article: found