- Record: found
- Abstract: found
- Article: found
Current strategies for the treatment of solitary and aneurysmal bone cysts: A review of the literature
Read this article at
Highlights
Abstract
This review of the literature aims to compare the etiology, the pathogenesis, the clinical diagnostics and the relevant treatment options of two different types of cystic bone lesions: the solitary bone cyst (SBC) and the aneurysmal bone cyst (ABC). Whereas the clinical symptoms and the radiographic appearance can be similar, the diagnostic pathway and the treatment options are clearly different.
The solitary bone cyst (SBC) represents a tumor-like bone lesion, occurring most frequently in the humerus and femur in children and adolescents. Pain caused by intercurrent pathological fractures is often the first symptom, and up to 87% of the cysts are associated with pathological fractures. In the majority of cases SBCs can be treated conservatively, especially in the upper extremity. However, if a fracture is completely dislocated, joint affecting, unstable or open, surgical treatment is necessary. Pain under weight bearing or regaining the ability to mobilize after fracture timely can necessitate surgical treatment in SBCs affecting the lower extremity. Spontaneous resolution can be seen in rare cases.
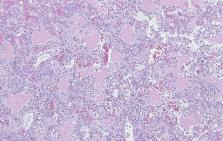
The aneurysmal bone cyst (ABC) is a benign, locally aggressive tumor that occurs in childhood and early adulthood. It usually affects the metaphysis of long bones but can also occur in the spine or the pelvis. ABC can be primary but also secondary to other bone pathologies. The diagnosis has to be confirmed by biopsy and histopathological examinations. With cytogenetic studies and the detection of specific translocations of the ubiquitin-specific protease (USP) 6 gene primary ABCs can be differentiated from secondary ABCs and other bone lesions. Among various modalities of treatment i.e. en bloc resection, intralesional curettage with adjuvants, embolization or the systemic application of denosumab, intralesional sclerotherapy using polidocanol is an effective and minimally invasive treatment of primary ABCs.
Related collections
Most cited references71
- Record: found
- Abstract: found
- Article: not found
USP6 and CDH11 oncogenes identify the neoplastic cell in primary aneurysmal bone cysts and are absent in so-called secondary aneurysmal bone cysts.
- Record: found
- Abstract: found
- Article: not found
Bone cysts: unicameral and aneurysmal bone cyst.
- Record: found
- Abstract: found
- Article: not found