- Record: found
- Abstract: found
- Article: found
Association of International Editorial Staff With Published Articles From Low- and Middle-Income Countries
Read this article at
Key Points
Question
Do medical journals whose editorial staff includes more editors affiliated with low- and middle-income countries (LMICs) publish more original research conducted in LMICs?
Abstract
Importance
The association between geographic diversity of medical journal editorial staff and publications reporting research conducted in low- and middle-income countries (LMICs) is unclear.
Objective
To examine the association between having editorial staff members affiliated with LMICs and publishing research articles from LMICs in leading biomedical journals.
Design, Setting, and Participants
This cross-sectional study included biomedical journals in fields representing the largest disease burden globally from January 1 to December 31, 2020. Websites of the 5 leading journals in general medicine, pediatrics, surgery, obstetrics and gynecology, cancer, cardiovascular diseases, infectious diseases, psychiatry, and nutrition were reviewed to obtain the country affiliations of editorial staff members. To determine article study countries, original research articles in each journal were reviewed through MEDLINE. Editorial staff country affiliations and study country locations were classified according to World Bank income brackets and regions.
Main Outcomes and Measures
Descriptive statistics of the proportion of editorial staff affiliated with each income bracket and region and Spearman rank correlation coefficients were used to assess the association between the proportion of editorial staff affiliated with LMICs and the proportion of published articles reporting work conducted in these countries.
Results
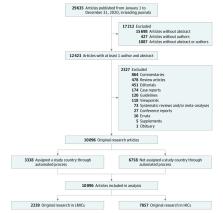
There were 3819 editorial staff members in the 45 included journals: 3637 (95.2%) were affiliated with high-income countries, 140 (3.7%) with upper-middle-income countries, 37 (1.0%) with lower-middle-income countries, and 5 (0.1%) with low-income countries. All 48 editors-in-chief were affiliated with a high-income country. Editorial staff members were mostly affiliated with North American countries (n = 2120 [55.5%]) and European or Central Asian countries (n = 1256 [32.9%]). Of the 10 096 original research articles included in our analysis, 7857 (77.8%) reported research conducted in high-income countries, 1562 (15.5%) reported research conducted in upper-middle-income countries, 507 (5.0%) reported research conducted in lower-middle-income countries, and 170 (1.7%) reported research conducted in low-income countries. Greater editorial staff representation correlated moderately with more published articles reporting research conducted in LMICs (Spearman ρ = 0.51; 95% CI, 0.25-0.70; P < .001).
Conclusions and Relevance
In this cross-sectional study, editorial staff in leading biomedical journals were largely composed of individuals affiliated with high-income countries in North America and Europe. A correlation was found between greater editorial staff representation and publication of research focused on LMICs, suggesting that the inclusion of editorial staff affiliated with LMICs may promote the publication of research conducted in those countries.
Abstract
This cross-sectional study examines the association of having editorial staff members affiliated with low- and middle-income countries with publications reporting research from low- and middle-income countries in leading biomedical journals.
Related collections
Most cited references24

- Record: found
- Abstract: found
- Article: found
Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019
- Record: found
- Abstract: found
- Article: not found
Building capacity in health research in the developing world.
- Record: found
- Abstract: not found
- Article: not found