- Record: found
- Abstract: found
- Article: found
Generic-reference and generic-generic bioequivalence of forty-two, randomly-selected, on-market generic products of fourteen immediate-release oral drugs
Read this article at
Abstract
Background
The extents of generic-reference and generic-generic average bioequivalence and intra-subject variation of on-market drug products have not been prospectively studied on a large scale.
Methods
We assessed bioequivalence of 42 generic products of 14 immediate-release oral drugs with the highest number of generic products on the Saudi market. We conducted 14 four-sequence, randomized, crossover studies on the reference and three randomly-selected generic products of amlodipine, amoxicillin, atenolol, cephalexin, ciprofloxacin, clarithromycin, diclofenac, ibuprofen, fluconazole, metformin, metronidazole, paracetamol, omeprazole, and ranitidine. Geometric mean ratios of maximum concentration (C max) and area-under-the-concentration-time-curve, to last measured concentration (AUC T), extrapolated to infinity (AUC I), or truncated to C max time of reference product (AUC Reftmax) were calculated using non-compartmental method and their 90% confidence intervals (CI) were compared to the 80.00%–125.00% bioequivalence range. Percentages of individual ratios falling outside the ±25% range were also determined.
Results
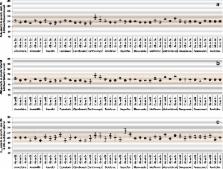
Mean (SD) age and body-mass-index of 700 healthy volunteers (28–80/study) were 32.2 (6.2) years and 24.4 (3.2) kg/m 2, respectively. In 42 generic-reference comparisons, 100% of AUC T and AUC I CIs showed bioequivalence, 9.5% of C max CIs barely failed to show bioequivalence, and 66.7% of AUC Reftmax CIs failed to show bioequivalence/showed bioinequivalence. Adjusting for 6 comparisons, 2.4% of AUC T and AUC I CIs and 21.4% of C max CIs failed to show bioequivalence. In 42 generic-generic comparisons, 2.4% of AUC T, AUC I, and C max CIs failed to show bioequivalence, and 66.7% of AUC Reftmax CIs failed to show bioequivalence/showed bioinequivalence. Adjusting for 6 comparisons, 2.4% of AUC T and AUC I CIs and 14.3% of C max CIs failed to show bioequivalence. Average geometric mean ratio deviation from 100% was ≤3.2 and ≤5.4 percentage points for AUC I and C max, respectively, in both generic-reference and generic-generic comparisons. Individual generic/reference and generic/generic ratios, respectively, were within the ±25% range in >75% of individuals in 79% and 71% of the 14 drugs for AUC T and 36% and 29% for C max.
Conclusions
On-market generic drug products continue to be reference-bioequivalent and are bioequivalent to each other based on AUC T, AUC I, and C max but not AUC Reftmax. Average deviation of geometric mean ratios and intra-subject variations are similar between reference-generic and generic-generic comparisons.
Related collections
Most cited references58
- Record: found
- Abstract: not found
- Article: not found
What's the price of a research subject? Approaches to payment for research participation.
- Record: found
- Abstract: found
- Article: not found
A review of the differences and similarities between generic drugs and their originator counterparts, including economic benefits associated with usage of generic medicines, using Ireland as a case study
- Record: found
- Abstract: found
- Article: not found